India alone accounts for more than 10% of gallbladder cancers worldwide. This makes India the world’s capital for gallbladder cancer. The prevalence of the cancer is especially high in Uttar Pradesh Bihar and the eastern states while it is fairly less in Western and Southern India. It is not really known what is the cause of the high incidence of gallbladder cancer in these specific parts of India. Some studies have shown a higher incidence of industrial waste and heavy metals in the water in the Gangetic belt, which could be one of the causative agents for the higher incidence of gallbladder cancers.
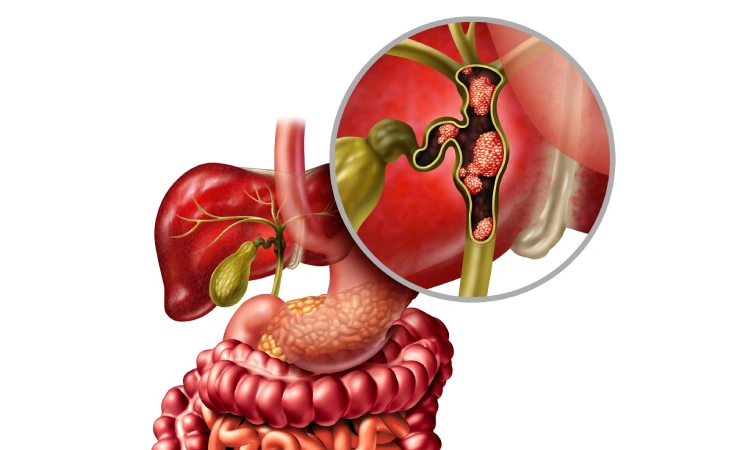
It is also interesting to know that 60- 80% of patients with gallbladder cancers in India have concomitant gallstone disease. Longstanding cholecystitis and gallstone disease. Maybe one of the contributing factors to this cancer.
We are a tertiary referral center for gallbladder cancers and we find a large number of patients where cancer has been incidentally detected in the pathology specimen of cholecystectomy for gallstone disease.
It does hence important for radiologists to be aware and report any abnormal thickening in the wall of the gallbladder in patients with gallstone disease which could be suspicious for gallbladder cancer.
One should not hesitate in such situations to carry out a triple-phase CT scan or an MRI to confirm or negate the possibility of gallbladder cancer.
Outcomes of gallbladder cancer surgery are much better when performed per premium rather than a revision surgery after the gallbladder has been removed.
If gallbladder cancer has been picked up upfront, the normal surgery would include the removal of the gallbladder with a wedge of the liver with a margin of around 2 cm from segments 4B and 5 along with the complete portal. Lymphadenectomy and the sampling of the cystic duct margin in the frozen section.
If the cystic duct shows evidence of cancer, the bile duct also may need to be resected.
Some patients with gallbladder cancer may need more major surgeries in the form of a bi-segmental liver section or even a right hepatectomy.
A vast majority of gallbladder cancers are however inoperable because they present to us in an advanced stage with metastases, either in the liver or the peritoneum or extensive lymph nodes. Many of these patients would then be eligible only for a palliative stenting if they are jaundiced followed by chemotherapy.
In view of the poor outcomes of this cancer, it is important to diagnose these cancers at an early stage so as to give these patients the best chance for survival.